Severe oral infections in children are uncommon but can become medical emergencies if they spread beyond the teeth and gums.
📌 Recommended Article :
Dental Article 🔽 Appropriate Antibiotic Use in Pediatric Odontogenic Infections: Guidelines for Dentists and Dental Students ... This article provides evidence-based, clinically practical guidance for dentists and dental students on the appropriate use of antibiotics in pediatric odontogenic infections.Most begin as untreated dental infections and may rapidly involve the facial spaces of the head and neck. Early recognition and prompt treatment greatly reduce the risk of serious complications.
Advertisement
This guide explains the most important forms of severe oral infection, their warning signs, treatment options, and when urgent medical attention is required.
✅ What Are Severe Oral Infections?
A severe oral infection occurs when bacteria spread from an infected tooth or surrounding tissues into the deeper spaces of the face, jaw, or neck.
The most important conditions include:
▪️ Odontogenic cellulitis
▪️ Deep facial space infections
▪️ Ludwig's angina
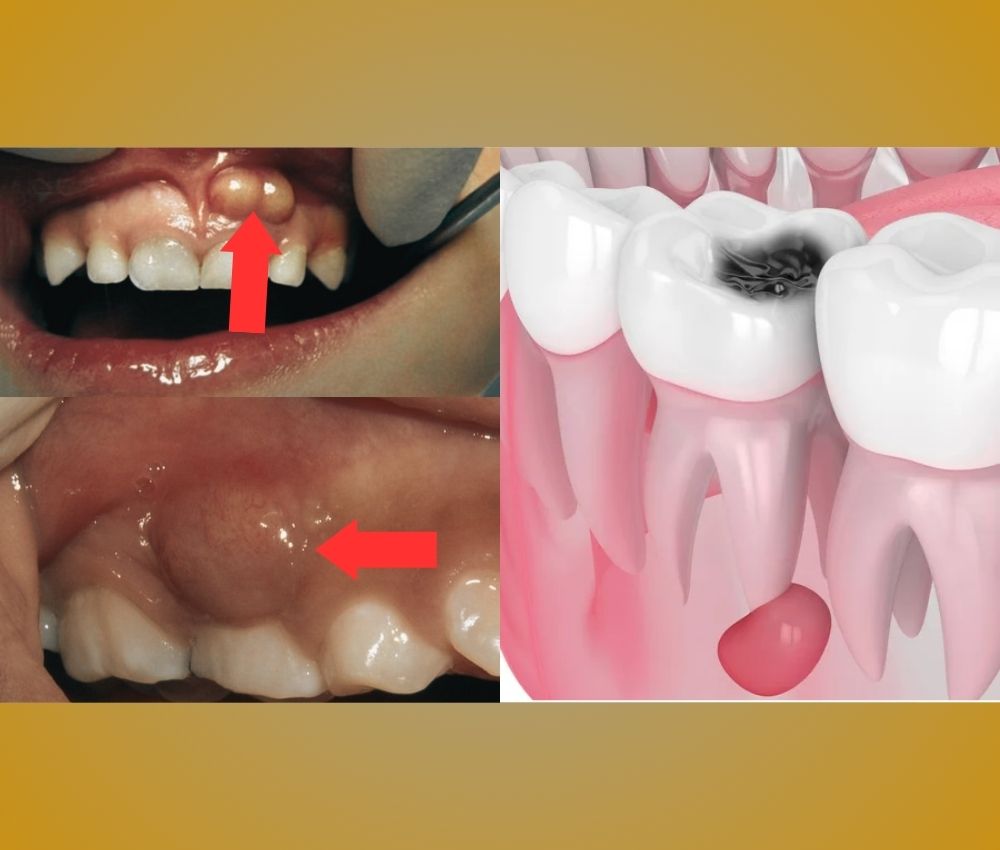
▪️ Dental abscesses with systemic involvement
Although these infections are primarily caused by bacteria commonly found in the mouth, delayed treatment allows them to spread rapidly.
📌 Recommended Article :
PDF 🔽 Management of acute orofacial infection of odontogenic origin in children - PDF Guide ... These infections often arise from untreated dental caries, pulp necrosis, or periodontal involvement and may rapidly spread through facial spaces due to the unique anatomical and immunological characteristics of pediatric patients.✅ Common Causes
The most frequent causes include:
▪️ Untreated dental caries
▪️ Dental abscesses
▪️ Advanced pulp infections
▪️ Dental trauma with pulp necrosis
▪️ Delayed dental treatment
▪️ Poor oral hygiene
Children with weakened immune systems may be at higher risk of developing severe infections.
📌 Recommended Article :
PDF 🔽 Odontogenic facial cellulitis in a pediatric patient - Diagnosis, treatment and multidisciplinary management ... Due to anatomical, immunological, and behavioral factors unique to children, these infections can progress quickly and may compromise vital structures, including the airway, orbit, or deep neck spaces.✅ Warning Signs
Parents should seek immediate dental or medical evaluation if a child develops:
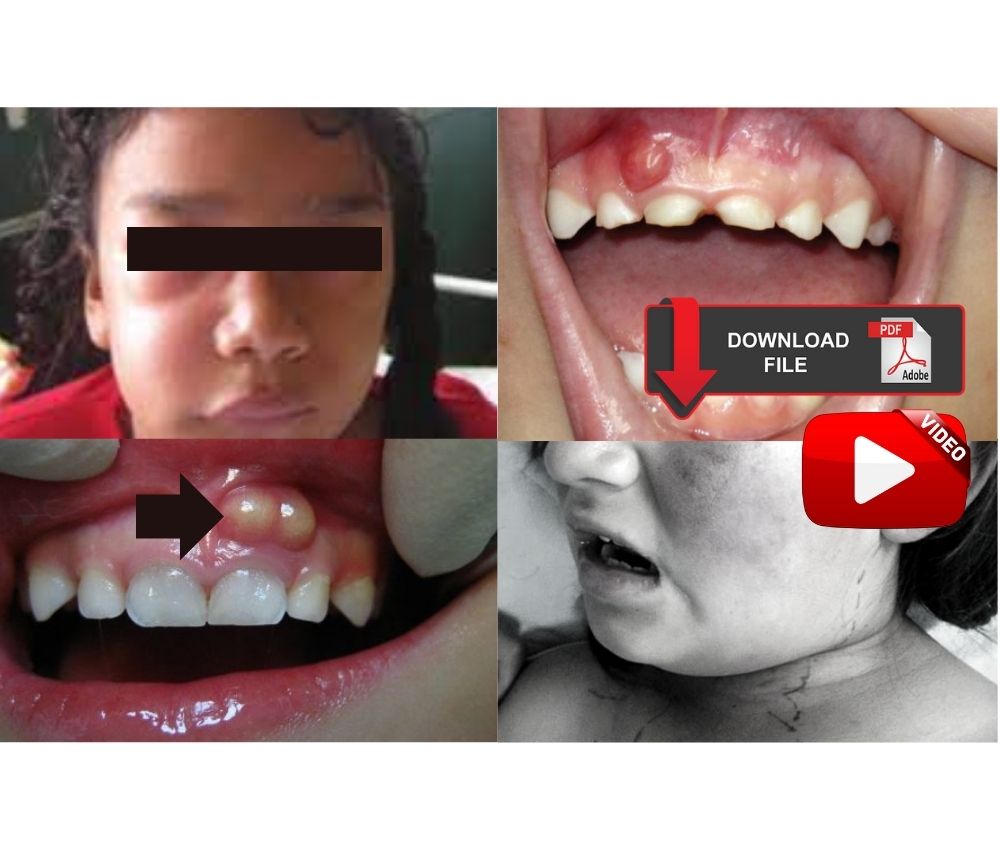
▪️ Rapid facial swelling
▪️ Severe toothache
▪️ Fever
▪️ Difficulty swallowing
▪️ Difficulty opening the mouth (trismus)
▪️ Difficulty breathing
▪️ Neck swelling
▪️ Fatigue or lethargy
Breathing difficulty is always an emergency.
📌 Recommended Article :
Dental Article 🔽 Facial Cellulitis vs. Angioedema in Dental Emergencies: Key Differences, Severity, and Management ... Dental professionals must be equipped to rapidly recognize the condition, initiate emergency management, and refer to a hospital setting when needed.✅ From Cellulitis to Ludwig's Angina
Cellulitis
Cellulitis is a diffuse bacterial infection that spreads through the soft tissues instead of remaining localized like an abscess.
Typical signs include:
▪️ Painful swelling
▪️ Redness
▪️ Warm skin
▪️ Fever
▪️ Rapid progression
Without treatment, cellulitis may spread into deeper facial spaces.
Ludwig's Angina
Ludwig's angina is one of the most dangerous odontogenic infections.
It is characterized by:
▪️ Rapid bilateral swelling beneath the jaw
▪️ Elevation of the tongue
▪️ Difficulty swallowing
▪️ Drooling
▪️ Muffled voice
▪️ Airway obstruction
Because the airway may become blocked, Ludwig's angina requires immediate hospital treatment.
📌 Recommended Article :
Dental Article 🔽 Management of Pulpal Infections in Primary Teeth: Evidence-Based Protocols ... This 2025 update provides a concise, evidence-based overview of pulpal infection management in primary teeth, following the latest AAPD 2024 classification and clinical protocols.✅ Diagnosis
Diagnosis is based on:
▪️ Complete medical and dental history
▪️ Clinical examination
▪️ Evaluation of airway involvement
▪️ Dental radiographs when appropriate
▪️ Contrast-enhanced CT imaging for suspected deep neck infections
Blood tests may be requested in severe systemic infections.
📌 Recommended Article :
Dental Article 🔽 Periapical Abscess vs Periodontal Abscess: Key Differences, Similarities, and Treatments ... Understanding their etiology, clinical manifestations, and treatment is essential for achieving predictable outcomes and avoiding complications.✅ Treatment
Management depends on the severity of infection.
Localized infections
▪️ Drainage of the abscess when indicated
▪️ Removal of the infection source
▪️ Appropriate antibiotics
▪️ Pain control
Severe infections
Children with facial cellulitis or suspected deep space infection often require:
▪️ Hospital admission
▪️ Intravenous antibiotics
▪️ Airway monitoring
▪️ Surgical drainage if necessary
▪️ Treatment of the infected tooth after stabilization
Early intervention significantly improves outcomes.
📊 Pharmacological Management of Severe Oral Infections in Children
| Medication | Clinical Use | Important Considerations |
|---|---|---|
| Amoxicillin | First-line oral antibiotic for mild to moderate odontogenic infections without systemic involvement. | Not appropriate for severe facial cellulitis requiring hospitalization. Dose should be adjusted according to the child's weight. |
| Amoxicillin–Clavulanate | Preferred for moderate to severe odontogenic infections when broader antibacterial coverage is needed. | Provides activity against beta-lactamase-producing bacteria. Gastrointestinal upset may occur. |
| Clindamycin | Alternative for children allergic to penicillins and effective against anaerobic bacteria. | Associated with an increased risk of Clostridioides difficile infection. Use only when clinically indicated. |
| Ampicillin–Sulbactam (IV) | Recommended for hospitalized children with facial cellulitis or deep odontogenic infections. | Requires intravenous administration and close hospital monitoring. |
| Ceftriaxone (IV) | May be used in selected hospitalized patients, often combined with anaerobic coverage. | Should be prescribed according to local antimicrobial guidelines and infection severity. |
| Metronidazole | Adjunctive therapy when enhanced anaerobic coverage is required. | Usually combined with another antibiotic rather than used alone for odontogenic infections. |
| Acetaminophen (Paracetamol) | First-choice analgesic and antipyretic for pain and fever control. | Does not treat the infection. Maximum daily dose should not be exceeded. |
| Ibuprofen | Provides analgesic, antipyretic, and anti-inflammatory effects in children without contraindications. | Use cautiously in dehydrated children or those with renal disease or gastrointestinal disorders. |
Without prompt treatment, severe infections may lead to:
▪️ Deep neck infections
▪️ Airway obstruction
▪️ Sepsis
▪️ Mediastinitis
▪️ Osteomyelitis
▪️ Hospitalization
▪️ Rarely, death
Fortunately, these complications are uncommon when treatment begins early.
📌 Recommended Article :
Dental Article 🔽 Dental Abscess, Fistula, Cellulitis, and Ludwig's Angina: Differences, Symptoms & Treatment ... Timely diagnosis, tailored antimicrobial therapy, and prompt referral to specialized care are key to reducing the risk of complications in odontogenic infections.✅ Prevention
The best prevention strategies include:
▪️ Regular dental check-ups
▪️ Early treatment of cavities
▪️ Daily tooth brushing with fluoride toothpaste
▪️ Healthy diet with limited sugar intake
▪️ Immediate evaluation of facial swelling or dental pain
Preventive dental care remains the most effective way to avoid severe odontogenic infections.
📌 Recommended Article :
Dental Article 🔽 Glass Ionomer Cement in Pediatric Dentistry: Benefits, Uses, and Step-by-Step Application Guide ... Glass ionomer cement (GIC) is a widely used dental material in pediatric dentistry due to its strong adhesion, fluoride release, and biocompatibility.💬 Discussion
Most severe oral infections in children originate from preventable dental disease. Although antibiotics are essential in selected cases, they do not replace definitive dental treatment, such as drainage or removal of the infection source.
The greatest clinical concern is recognizing signs of airway compromise, particularly in children with rapidly progressing swelling or suspected Ludwig's angina. Close collaboration between pediatric dentists, oral and maxillofacial surgeons, pediatricians, and emergency physicians is often necessary to ensure safe and effective care.
🎯 Recommendations
▪️ Never ignore facial swelling associated with tooth pain.
▪️ Seek emergency care immediately if breathing or swallowing becomes difficult.
▪️ Complete the full course of prescribed antibiotics.
▪️ Attend regular dental examinations.
▪️ Treat dental decay before complications develop.
▪️ Educate parents about the warning signs of spreading dental infections.
✍️ Conclusion
Severe oral infections in children can progress quickly from localized cellulitis to life-threatening conditions such as Ludwig's angina. Early diagnosis, prompt dental intervention, appropriate antibiotic therapy, and timely hospital management are essential for preventing serious complications. Maintaining good oral hygiene and treating dental disease early remain the most effective preventive measures.
📚 References
✔ American Academy of Pediatric Dentistry. (2024). Use of antibiotic therapy for pediatric dental patients. The Reference Manual of Pediatric Dentistry. Chicago, IL: American Academy of Pediatric Dentistry.
✔ American Association of Endodontists. (2021). AAE guidance on the use of systemic antibiotics in endodontics. Chicago, IL: American Association of Endodontists.
✔ Flynn, T. R.. (2011). Severe odontogenic infections. Oral and Maxillofacial Surgery Clinics of North America, 23(3), 401–413. https://doi.org/10.1016/j.coms.2011.04.001
✔ National Institute for Health and Care Excellence. (2020). Dental abscess: antimicrobial prescribing (NG187).
📌 More Recommended Items
► Key Differences Between Pediatric and Adult Odontogenic Infections: Updated Clinical Guidelines
► Odontogenic Infections in Children: Updated Diagnosis, Treatment and Prevention Guidelines
► Antibiotic Selection in Pediatric Dental Infections: Updated Clinical Criteria for U.S. Dentists