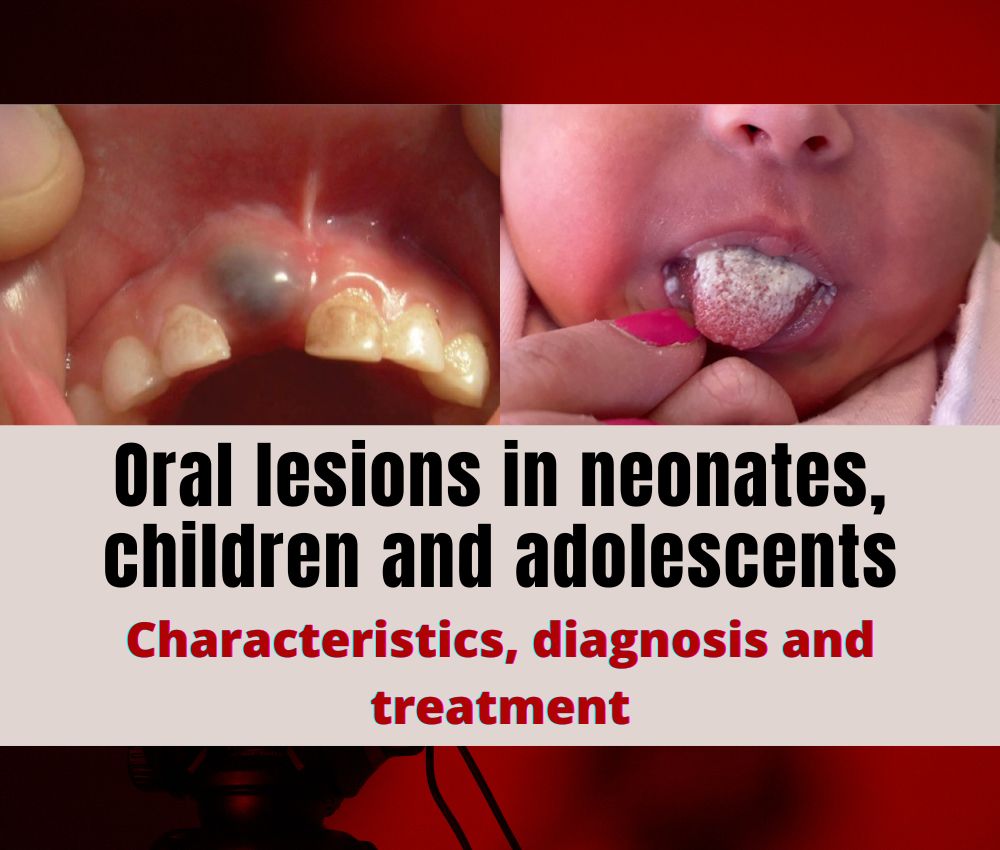
Mucocele is a benign lesion that occurs in the oral mucosa and is the product of an alteration in the minor salivary glands. It is recognized as a swelling with mucous content, well circumscribed, and bluish in color.
📌 Recommended Article :
PDF 🔽 Marsupialization of a large mandibular cyst in a pediatric patient - Clinical Case ... Various techniques are used to surgically remove the mandibular cyst, enucleation when the cyst is small, or marsupialization when it is large
The presence of a mucocele may be due to trauma or ductal obstruction. The treatment is surgical and anesthesia is local, but depending on the behavior of the pediatric patient it can be performed with general anesthesia.
Advertisement
Let's know the clinical and pathological characteristics of salivary mucocele in children and adolescents.
📌 Recommended Article :
PDF 🔽 Surgical excision of mucocele with local anesthesia in an 8-month-old baby ... We share the case of the surgical removal of a mucocele in an 08-month-old baby under local anesthesia
📌 Read and download the article in PDF 1:
Poulopoulos A, Andreadis D, Parcharidis E, Grivea I, Syrogiannopoulos G, et al. (2017) Salivary Mucoceles in Children and Adolescents: A Clinicopathological Study. Glob J Medical Clin Case Rep 4(1): 011-014. DOI: 10.17352/2455-5282.000035
📌 Read and download the article in PDF 2:
Lewandowski B, Brodowski R, Pakla P, Makara A, Stopyra W, Startek B. Mucoceles of minor salivary glands in children. Own clinical observations. Dev Period Med. 2016;20(3):235-242. PMID: 27941195.
📌 More Recommended Items
► Natal teeth and Riga Fede ulcer: Diagnosis and treatment
► Management of antibiotics in odontogenic infections in pediatric dentistry
► Guideline on Pediatric Oral Surgery